
CASE REPORT : THE HEART BOMB Submitted by : Dr Mohammad Najeebuddin
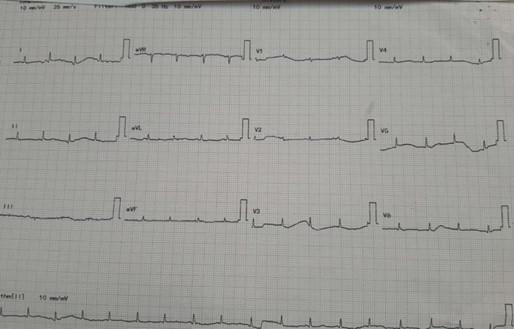
Large pericardial effusion with impending cardiovascular collapse is a differential diagnosis to be considered in a patient presenting with highly unstable vitals with severe shortness of breath and tachypnea. Point of care ultrasonography helps to catch the diagnosis and intervene immediately to save a life. Pericardiocentesis is an essential skill to be learnt by doctors working in the emergency department. A 25-year female with no known comorbidities was brought to the ED with severe breathlessness. Patient was connected to a cardiac monitor. She was conscious and oriented . The vitals were recorded as heart rate 116 bpm, BP 170/100 , SpO2 97% on room air and this had started one month back, insidiously progressed to grade IV . The attendants informed that she is not able to lie supine from one day because of shortness of breath. We enquired about fever,cough and chest pain which were absent. Patient had bilateral pedal edema from 15 days which had progressed to generalized edema over the last 2 days. There was a history of anorexia and significant weight loss over the last one month . The patient had no complaints of oliguria, jaundice, rash , joint pains or oral ulcers. Physical examination revealed distended neck veins , pallor , pedal edema extending upto thigh level, normal heart sounds and crepitations in bilateral infra-axillary regions. Our working differentials were looking for an underlying cardiac, respiratory or malignant cause for acute presentation of this patient. We ordered an ECG (Figure 1) which showed Sinus tachycardia with normal axis and Low voltage complexes in both limb and chest leads. ABG reported a compensated High Anion Gap Metabolic Acidosis with lactates of 3.5 and Hemoglobin of 7.1. POCUS cardiac views- Parasternal long axis and Apical views were performed. Figure 2 shows a Large circumferential pericardial effusion with right ventricular diastolic collapse . There was no chamber dilatation, vegetations or clots. LVEF was more than 50% and IVC diameter was 2.1 without respiratory variability. Figure 1. Figure 2. M mode ultrasound showing diastolic collapse of right ventricle. From the above findings the patient was diagnosed to be in cardiac tamponade. Immediate cardiology consultation was taken . Patient was initiated on continuous cardiac monitoring, O2 supplementation at 10 L/min, 500 ml Normal saline was infused. The Blood bank was informed to reserve one unit of cross matched packed red cells .The patient was deteriorating fast and we planned emergency pericardiocentesis . Informed written consent was taken and pericardiocentesis tray was prepared . Under USG guidance and aseptic precautions, the subxiphoid approach was used to gain access to the pericardial space. Saline echo contrast test using agitated saline was used to sonographically confirm the position of the 7 Fr catheter in the pericardial space. 250 ml of sero-sanguineous fluid was drained by serial aspiration using a 50ml syringe connected to the pigtail catheter now in-situ, which was fixed using 2 ‘0 silk and sterile tegaderm dressing. Post pericardiocentesis vitals were heart rate of 104, BP of 150/90, R R of 24 and SpO2 of 94%. Repeat POCUS showed absence of right ventricular diastolic collapse and moderate pericardial effusion. The pericardial fluid samples were sent for biochemical, cytological and microbiological analysis with help of the cardiology team. Patient was admitted under cardiology and shifted. Figure 3. M mode ultrasound image post pericardiocentesis not showing any right ventricular diastolic collapse. Follow up of the patient showed Hb of 5.6 mg/dl with microcytic hypochromic picture with platelet count of 1.2 lakh per . Thyroid profile revealed TSH of 10.34μIU/ml (Ref range 0.2-4μIU/ml). Pericardial fluid showed ADA level of 9.1 (>36 suggestive of TB). The ANA panel was ordered, rheumatology consultation was taken and the patient was provisionally diagnosed with non-specific connective tissue disorder. Patient was started on immunosuppressants, steroids and discharged after 20 days to follow up in the rheumatology OPD. DISCUSSION: The etiology of pericardial effusions (moderate to large) requiring pericardiocentesis varies a lot across various studies. A 2017 study by Strobbe et al from the Journal of American Heart Association, found malignant and idiopathic effusions to be the two most common causes (~25% each). The rest were divided among iatrogenic, infective, uremic and collagen vascular diseases.1 The effusions are graded for severity based on the size of anechoic shadow surrounding the heart on TTE. Moderate effusions are less than 1 cm in depth circumferential around the heart whereas large effusions are more than 1 cm. 2 Once tamponade is suspected, clinically multiple echocardiographic features are useful to confirm the same. These are- Late diastolic right atrial (RA) collapse: Signifies rise in intrapericardial pressure over the relatively low RA pressure. Inversion of the free wall of the right atrium for more than one third of the systole has 94% sensitivity and 100% specificity for the diagnosis of tamponade. Early diastolic RV collapse RV collapse is more specific but less sensitive compared to RA collapse for hemodynamically significant pericardial compression. It may not be seen in cases where the RV pressures are elevated due to prior pathology. M mode performed through the mid ventricle from the parasternal long axis view (as shown above) or short axis view gives better temporal resolution and aids in diagnosis. Plethora of the IVC with blunted respiratory changes due to the raised right sided pressures consequent to tamponade. It is often >2cm with <50% respiratory variation. Respiratory variation of mitral and tricuspid inflow: A decrease in mitral inflow velocity ‘E’ using the pulse wave (PW) doppler of >25% and increase of tricuspid inflow velocity >50%, both during the inspiratory phase suggest cardiac tamponade.3 There are three approaches by which pericardiocentesis may be performed: subxiphoid, apical and least commonly the parasternal. The apical approach requires the shortest distance traversed to reach the pericardial space. But with a higher risk of left ventricular puncture and iatrogenic pneumothorax, although the risk of the latter can be minimized with the use of ultrasound.With the subxiphoid approach the path to reach the fluid is longer, with risk of entry into the peritoneal
International First Aid Day

International First Aid Day serves as a poignant reminder of the pivotal role that immediate assistance plays in saving lives during emergencies. Observed globally on the second Saturday of September, this day underscores the significance of being the “first line of hope and help.” First aid knowledge empowers individuals to respond swiftly and effectively to injuries or sudden illnesses, bridging the crucial gap between the occurrence of an incident and the arrival of professional medical assistance. It highlights the importance of cultivating a society where everyone is equipped with the skills to provide basic medical care, fostering a community of caregivers ready to act in times of need. On this day, communities, organizations, and individuals come together to raise awareness, share knowledge, and celebrate the unsung heroes who serve as the initial lifeline in times of crisis. International First Aid Day is a call to action, urging people to be proactive contributors to the well-being of their communities, thereby reinforcing the notion that everyone can make a difference when it matters most. Download PDF
OPTIMIZING SEPSIS CARE IN EMERGENCY MEDICINE

Sepsis, often referred to as the silent killer, represents one of the most pressing challenges faced by emergency medical professionals worldwide. It is a condition that knows no boundaries, striking both the young and old, the previously healthy and the chronically ill. Our collective goal is to illuminate the path forward, to bridge the gap between evidencebased medicine and real-world practice, and to provide a platform for open discourse and shared experiences. Together, we aim to empower healthcare professionals with the knowledge, tools, and insights needed to deliver the highest standard of care to sepsis patients who entrust us with their lives. National Faculties Dr. Ashima Sharma Prof & HOD EMD ( NIMS Hyderabad) Dr. Bhavesh Jarwani Prof & HOD EMD (NHL Municipal Medical College Gujarat) Dr. Chandni Sajeevan HOD EMD (Government Medical College- Kozhikode Kerala) Dr. C R K Prasad Prof & HOD EMD (AIMSR Hyderabad) Dr. Harsha Makwana Prof & HOD EMD (LG hospital Narendra Modi Medical college Ahmedabad Gujarat Dr. Mehul Gujjar Assoc. Prof EMD (LG hospital Narendra Modi Medical college Ahmedabad Gujarat) Dr. Nidhi Kaeley Head EMD (AIIMS Rishikesh) Dr. Rashmi Sharma Prof & HOD EMD (SMS&R Sharda University GreaterNoida Dr. S. Prakash Babu Assoc. Prof EMD (St. Peters Medical College Hospital & Ri, Hasur, Tamiinadu) Dr. Varsha Shinde Prof & HOD EMD (DY Patil Medical College Pune) Dr. Varun Byrappa Assoc. Prof & HOD EMD (KIMS, Bengaluru) International Faculties Dr. Arunachalam Einstein MD, FACEP, FAAEM, Seattle, USA Dr. Venkat Kotam Raju FRCEM, MRCS, MdAcadMED, (Royal Derby Hospital UK) View and Download the PDF Download PDF
ZERO SNAKE BITE DEATHS :: IMPOSSIBLE TO POSSIBLE.

India is World’s ‘Snakebite Capital’ with 2.8 million bites a year with 35,000–50,000 people dying per year according to World Health Organization (WHO) [1,2]. Lack of a coordinated comprehensive care in snake bite management is the key factor of highest numbers of deaths and morbidity in India.India and our state, Assam too lacks comprehensive care model in snake bite management.However we ,Assam has no robust data about snake bite related deaths. We received phone calls from Digboi on 11/06/2022,patient was bitten by a snake ,they went to faith healer/tantra and mantra and died.They did not reported hospital.How many deaths are happening like this without notification to health centre,we donot have data. There is no LINK between snake bite and hospital care.Therefore we tried our best to create and sustain this link. Till 11th June of 2022,we have received reports of 3 deaths from various parts of Assam. Two were from Digboi and one was from Dhuburi.Unfortunately all these deaths could have been prevented if both public and health care workers were aware of venomous snake bite symptoms. For successful care of snake bite victims,we have to formulate comprehensive care to such victims,so that they shouldnot dissatisfied from our care.We also have to remember that snake bite is a poor men’s acute emergency.Therefore,we must try our best not to give economic burden to these poor patients in this snake bite crisis time. Therefore Comprehensive care is a planned coordinated preventive,promotive,curative,mental & socioeconomic care to snake bite victims. India lacks the coordinated movement of snake bite victims from field to hospital.Demow Model hospital cum CHC,tried their best to provide Comprehensive care to these victims since 2018. Why India need comprehensive care? 1.Lack of awareness amongst public. 2.Majority attended faith healers [3,4]. 3.Poorly trained health care workers (HCW) in rural districts [5,6]. Fear of HCW to administer ASV (Anti snake Venom). 4.Poor transportation system to hospital. 5.Delayed ASV administration [7,8] 6.Nonavailability of ASV 7.No support to victim’s family due to huge financial burden [9], if treatment is prolonged. 8.No address to mental issues post snake bite [10] 9.It is not approached as acute emergency. 10.Myth that snake bite cases can be treated only in tertiary center. India and Assam have huge gaps from prehospital, point of source hospital, secondary care hospital to Government level. For effective treatment of snake bite victims, we should have an organized care system. Prehospital management: Venom Response Team (VRT) Prehospital management is greatly neglected in India due to lack of education of our society. After snake bite our public completely lost and often misleaded. We started to train and educate public since 2008(Fig A). A VRT can be constructed to guide snake bite victims in each gram panchayat level comprising gram Sevak, local organizations & ASHA workers. They can be trained so that they can activate, communicate HCW & can transfer victims safely to nearest hospital. It is the need of the hour. Our model focused to educate, empower, and train public. These trained/educated public are called VRT.We have done till now 150 numbers of community awareness programme in and around Demow and Sibsagar district.We have also collaborated with APADA MITRA project of central Government under District Disaster Managaemner Society(FigB).Our plan is to create train and educate health volunteers under APADA Mitra Project,which are now officially called VRT.We have formed a whats app group with Public of different communities along with trained APADA MITRA health volunteers.These VRT will notify us as well as safe and scientifically transfer snake bite victims to nearby hospital. Figure: A: Community Awareness programme Our effort towards comprehensive care in snake bite in Upper Assam It is true that public and society have to rush to hospital once there is any snake bite. If they don’t rush to hospital immediately, morbidity and mortality couldn’t be prevented at all. So, our model starts from public/society and ends in Hospital. Public awareness & Education is the key. How we did it? We have to take help of 3Ps.Public, Press & Politician. Now a days, digital platform is the best to reach out many within short span of time. We have to publish our own successful stories in our own local language in various digital formats. Facebook and what’s app are the most popular digital media in various nook and corners of India, we should post our success stories of venomous snake bite treatments with photographs and address of the victim (with their written informed consent) . Let public know that snake bite means hospital admission. Make them believe that there is a full proof medical management of venomous/nonvenomous snake bite in India. We have also participated in Television talk show and Radio talk show campaigning for hospital admission immediately after snake bite. We have formed a what’s app group with our trained and educated general public. The name of our group is SNAKE: Public awareness group. It works like VRT. Every small community should have such group. We are readily accessible, and we come to know any snake bite incident in our local area, who are immediately transferred to nearby hospital. On 29th September 2019, we have conducted a scientific CME(Continuing Medical Education) about snake bite with our local public and General Practitioners. We have trained general public along with doctors, paramedical staff & ASHA workers. Strengthening the health care system We have interviewed 100 victims of snake bite all over from Assam. We found all had full faith in local healers and they believed there is no medical treatment for snake bite. Few of them reached nearest hospital at the earliest but soon referred from one hospital to other and died in the ambulance itself. Many hospitals had ASV but did not administered by health care workers for possibilities of litigation and fear. Few had expired ASV, and many hospitals did not have the ASV at all. We have also witnessed nearby hospitals were 100-200 km apart and, in some places, transportation was also not feasible. We have to strengthen our rural primary (PHC)